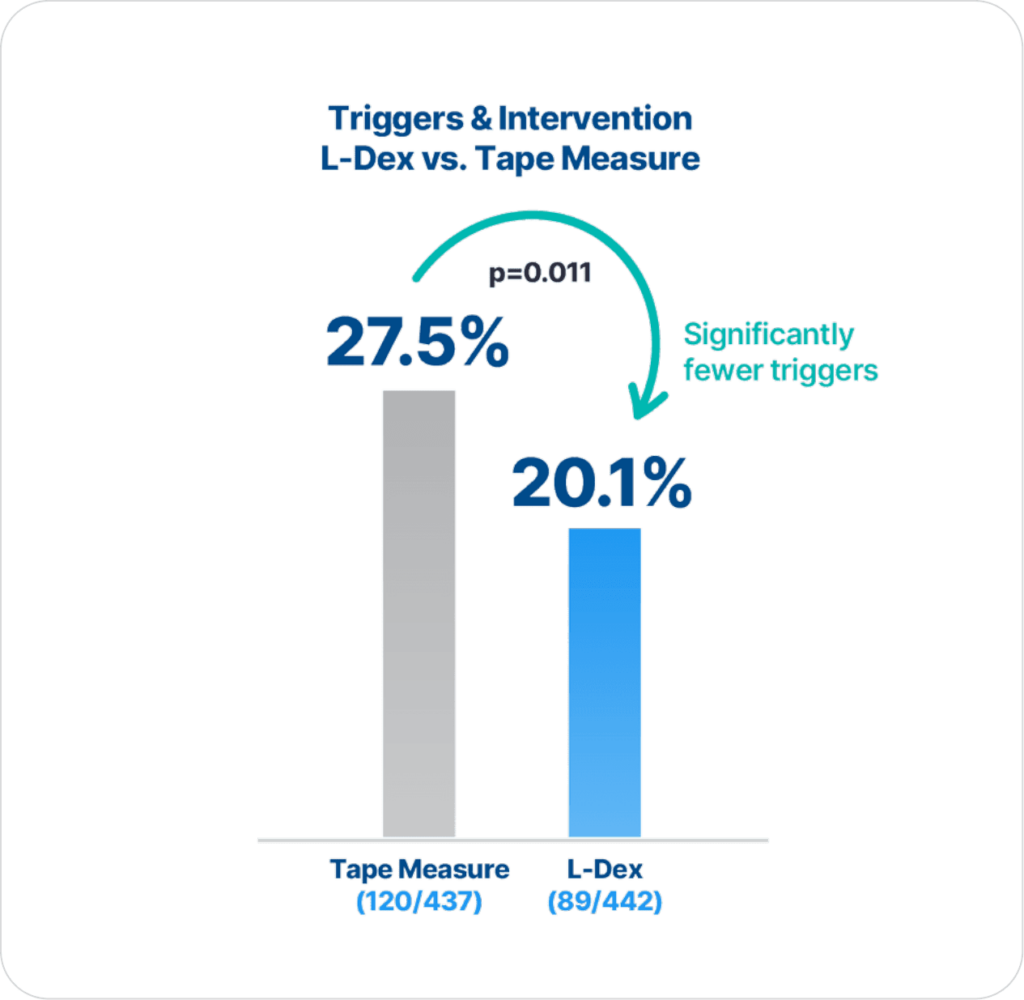
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
Extensive clinical evidence shows that using ImpediMed’s bioimpedance spectroscopy (BIS) technology for early detection and intervention reduces the impact of chronic lymphedema on breast cancer patients.
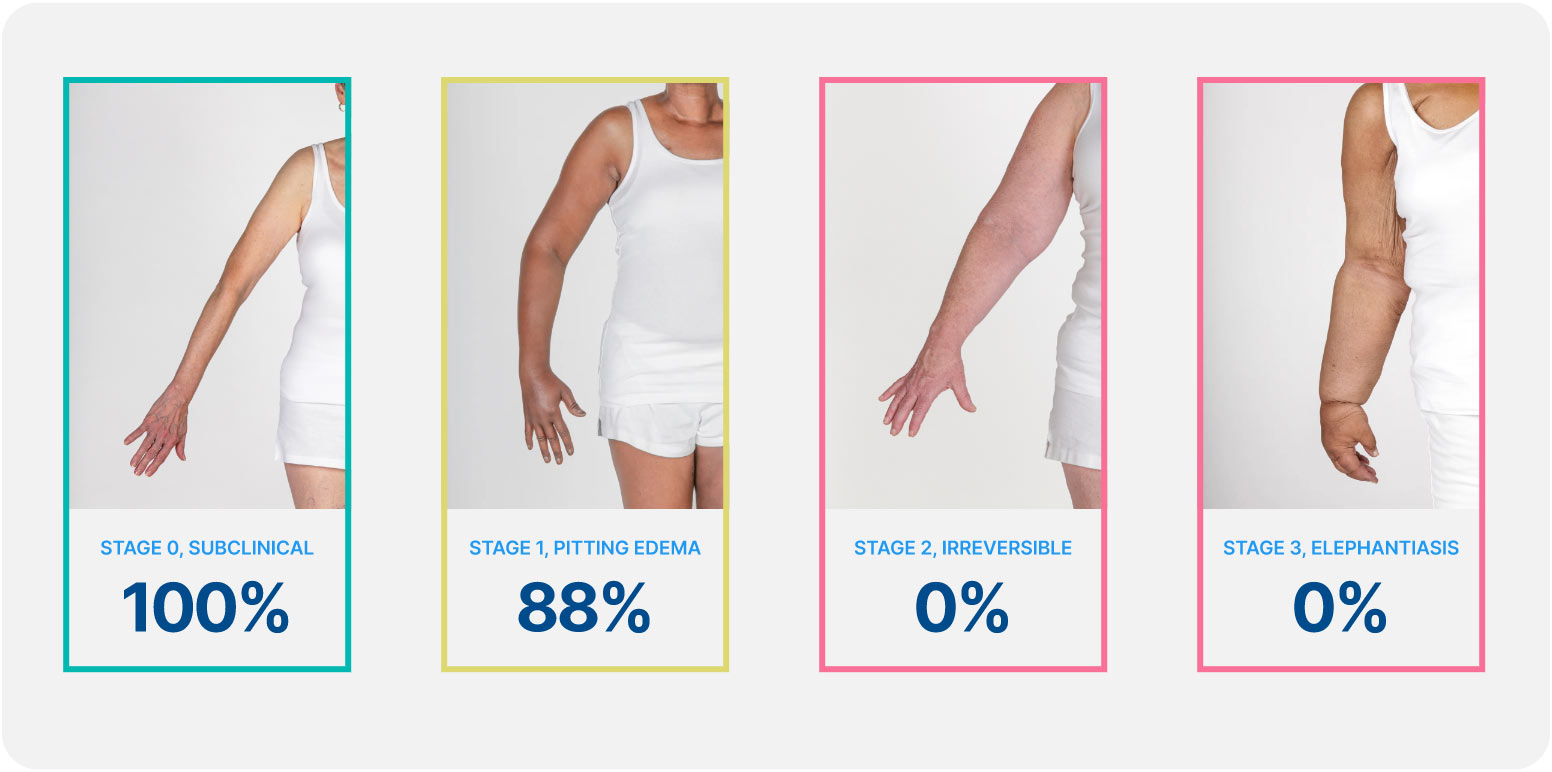
Lymphedema develops in stages, and a university of Kansas study found that when lymphedema is detected at stage 0 or stage 1 it is reversible, but in stages 2 and 3 it is not. These findings demonstrate how early conservative intervention and prospective monitoring with BIS can significantly lower rates of BCRL and persistent BCRL (pBCRL).¹
The PREVENT Trial involved 10 centers across the US and Australia and was the largest randomized controlled trial (RCT) to assess lymphedema prevention in breast cancer patients.
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
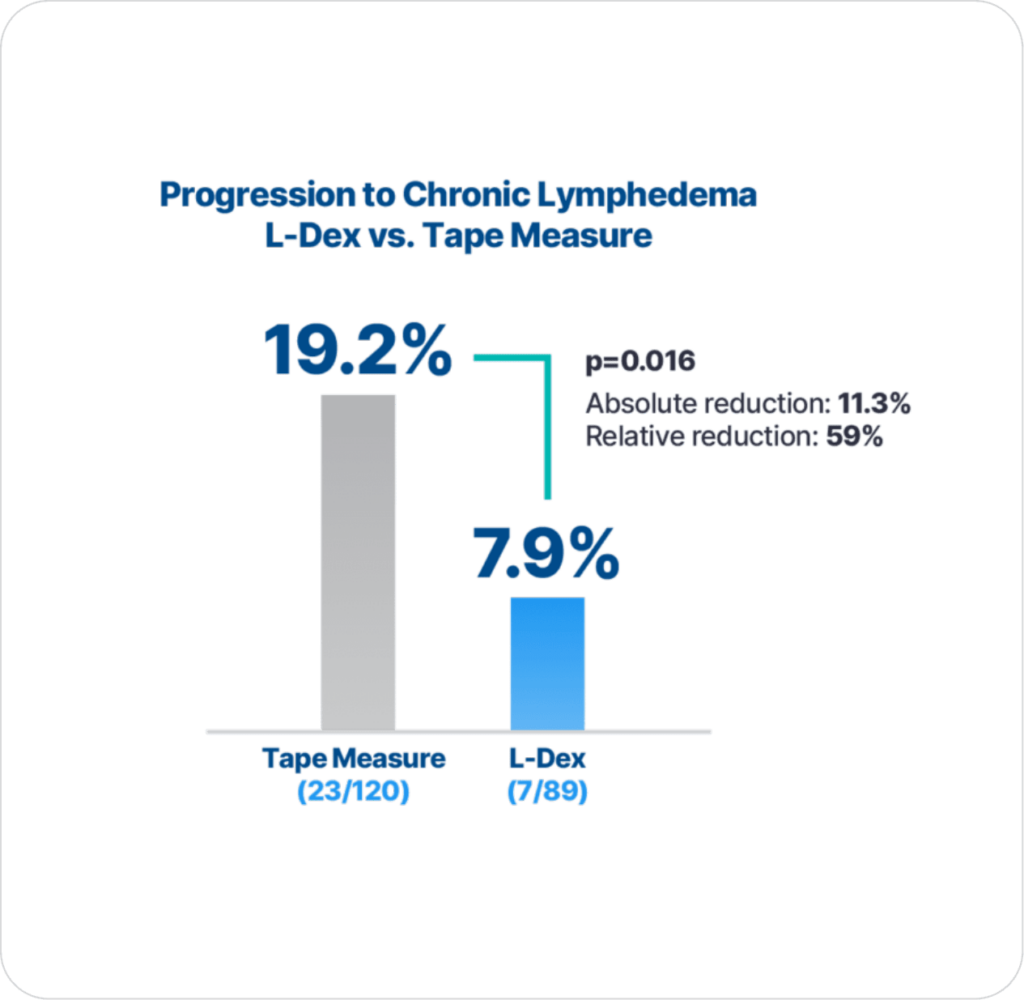
Additionally, with early detection using BIS technology and intervention there is significantly lower progression to chronic lymphedema compared to using tape measure (p=0.016), which is the primary endpoint result2.
Our results demonstrated that early conservative intervention for breast cancer patients high risk for BCRL who were prospectively monitored by utilizing BIS significantly lowers rates of BCRL. These findings support early prospective screening and intervention for BCRL. Early detection with patient-directed interventions improves patient outcomes and decreases the risk of persistent BCRL.
Kilgore, L.J., et al., Reducing Breast Cancer-Related Lymphedema (BCRL) Through Prospective Surveillance Monitoring Using Bioimpedance Spectroscopy (BIS) and Patient Directed Self-Interventions. Ann Surg Oncol, 2018.
The results of this analysis underscore previously published data on the efficacy of prospective BCRL surveillance and early intervention using BIS. Of the 93 high-risk patients prospectively followed and managed in this structured BCRL protocol, only 11% required CDP and only 3% required continued therapy. These excellent outcomes are superior to contemporary studies of conventional measures reporting BCRL rates in similarly treated high-risk patients.
Whitworth, P.W., et al., Preventing Breast Cancer-Related Lymphedema in High-Risk Patients: The Impact of a Structured Surveillance Protocol Using Bioimpedance Spectroscopy. Front Oncol, 2018. 8: p. 197.
STANDARD 2.15 – Support and Rehabilitation
Supportive services may include:
• Lymphedema management and risk reduction practices
RESOURCES
National Accreditation Program for Breast Centers (NAPBC) Accreditation Resources,
facs.org/quality-programs/napbc/accreditation/resources
Resource links to NLN guidelines
In summary, BIS represents a valuable and practical tool for the early detection of subclinical BCRL in patients undergoing prospective monitoring. In this prospective surveillance study, use of BIS allowed for early intervention and a reduction in the predicted rate of chronic BCRL compared to historical controls (no cases of persistent, chronic BCRL were observed after early intervention even in the highest risk patients). Such an approach represents not only a valuable strategy to address the recent NCCN guidelines on survivorship for monitoring for BCRL but also a cost-effective strategy to prevent and manage the potentially devastating effects of chronic BCRL.
Kaufman, D.I., et al., Utilization of bioimpedance spectroscopy in the prevention of chronic breast cancer-related lymphedema. Breast Cancer Res Treat, 2017. 166(3): p. 809-815.
In summary, prospective surveillance of breast cancer patients (most of whom were considered high risk) for the development of BCRL using BIS permitted the detection and simple pre-emptive management of subclinical disease resulting in a very low rate of chronic lymphedema compared to the established, expected range. These findings (which represent the largest group of patients monitored in a structured, program for early detection of BCRL using BIS) support the cost-effective allocation of resources for prospective, BIS assisted, BCRL surveillance within guidelines-based breast cancer survivorship programs. For women at risk for BCRL, this protocol represents a useful option to meet NCCN guidelines for the education, monitoring and treatment of BCRL.
Whitworth, P.W. and A. Cooper, Reducing chronic breast cancer-related lymphedema utilizing a program of prospective surveillance with bioimpedance spectroscopy. Breast J, 2018. 24(1): p. 62-65.
Practice Recommendations Based on Patient Presentation At Risk/Early Upper Extremity Lymphedema (ILS Stage 0-I)
Bioimpedance analysis (BIA) should be used to detect subclinical/early stage lymphedema (Grade B)
– Cutpoint of >7.1 L-Dex score should be used for diagnosis of breast cancer–related lymphedema when preoperative baseline measures are not available (Grade B)
– Cutpoint of >10 L-Dex score above preoperative baseline should be used for diagnosis of breast cancer–related lymphedema (Grade B)
– Preoperative assessment using BIA may enhance the ability to detect changes in tissue fluid earlier indicating lymphedema (Grade B)
A protocol for BIS via the L-Dex device should be established in clinical practice; this provides APNs with a consistent, objective approach to detect subclinical lymphedema, assists the APN with evidence-based decision making for PT referral, and provides improved lymphedema education from the APN for at-risk survivors. The protocol could decrease clinical lymphedema incidence, improving functional ability and quality of life among survivors by decreasing arm edema and reducing joint and muscle aches, limb tightness, infection rates, and overall medical costs for chronic lymphedema treatment.
Open access: NoThe results of this retrospective study demonstrate that L-Dex assessments can be incorporated into routine breast cancer programs as part of follow-up. This is critically important given the recent changes in the NCCN survivorship guidelines for post-treatment follow-up care for breast cancer patients establishing that health-care providers “educate, monitor, and refer for lymphedema management.” Additionally, the analyses suggest that L-Dex assessments can identify subclinical BCRL and subsequently monitor the return to baseline following conservative interventions. Further studies are required to demonstrate the long-term benefits of early detection and subsequently early intervention predicated upon subclinical detection of BCRL.
Laidley, M., Alison and M. Anglin, Beth, The Impact of L-Dex® Measurements in Assessing Breast Cancer Related Lymphedema (BCRL) as Part of Routine Clinical Practice. Frontiers in Oncology, 2016. 6(192).
With increasing data supporting early detection and treatment of BCRL, BIS has emerged as an important diagnostic modality due to its ability to detect subclinical lymphedema. BIS can be utilized as part of routine breast cancer clinical care starting with measurements prior to locoregional therapy and continued as part of survivorship using an increase of 10 to trigger early herapy for BCRL.
Open access: NoThis is the first study to establish evidence-based diagnostic criteria for LE against an appropriate reference standard. The two thresholds with the highest sensitivity, as well as good specificity, for detection of mild LE were determined from a normative population, accounting for normal inter-limb variations as well as limb dominance. These findings support the adoption of a more liberal diagnostic threshold set at 2SD above the mean, instead of the previously suggested 3SD threshold.
Dylke, E.S., et al., Diagnosis of upper limb lymphedema: development of an evidence-based approach. Acta Oncol, 2016: p. 1-7
Breast cancer-related lymphedema (BCRL) has become an increasingly important clinical issue as noted by the recent update of the 2015 NCCN breast cancer guidelines which recommends to “educate, monitor, and refer for lymphedema management.” The purpose of this review was to examine the literature regarding early detection and management of BCRL.
Several studies were identified that demonstrate that newer diagnostic modalities (bioimpedance spectroscopy, perometry) have increased sensitivity allowing for the earlier detection of BCRL. Current data support the development of surveillance programs geared toward the early detection and management of BCRL in part due to newer, more sensitive diagnostic modalities.
Open access: YesComplicated lymphedema was defined as any hospital admission within 2 years for a diagnosis of lymphedema or related complications based on prior research.
This study demonstrates a 2.3% incidence of complicated lymphedema after breast cancer surgery. Increased health care utilization for these patients resulted in hospital charge accrual of more than $180 million in 2 years or approximately $140,000 per patient. Although limitations must be taken into consideration, the significant burden of lymphedema underscored here mandates further investigation into targeted, anticipatory management strategies for BCRL
Basta, M.N., et al., Complicated breast cancer-related lymphedema: evaluating health care resource utilization and associated costs of management. Am J Surg, 2016. 211(1): p. 133-41.