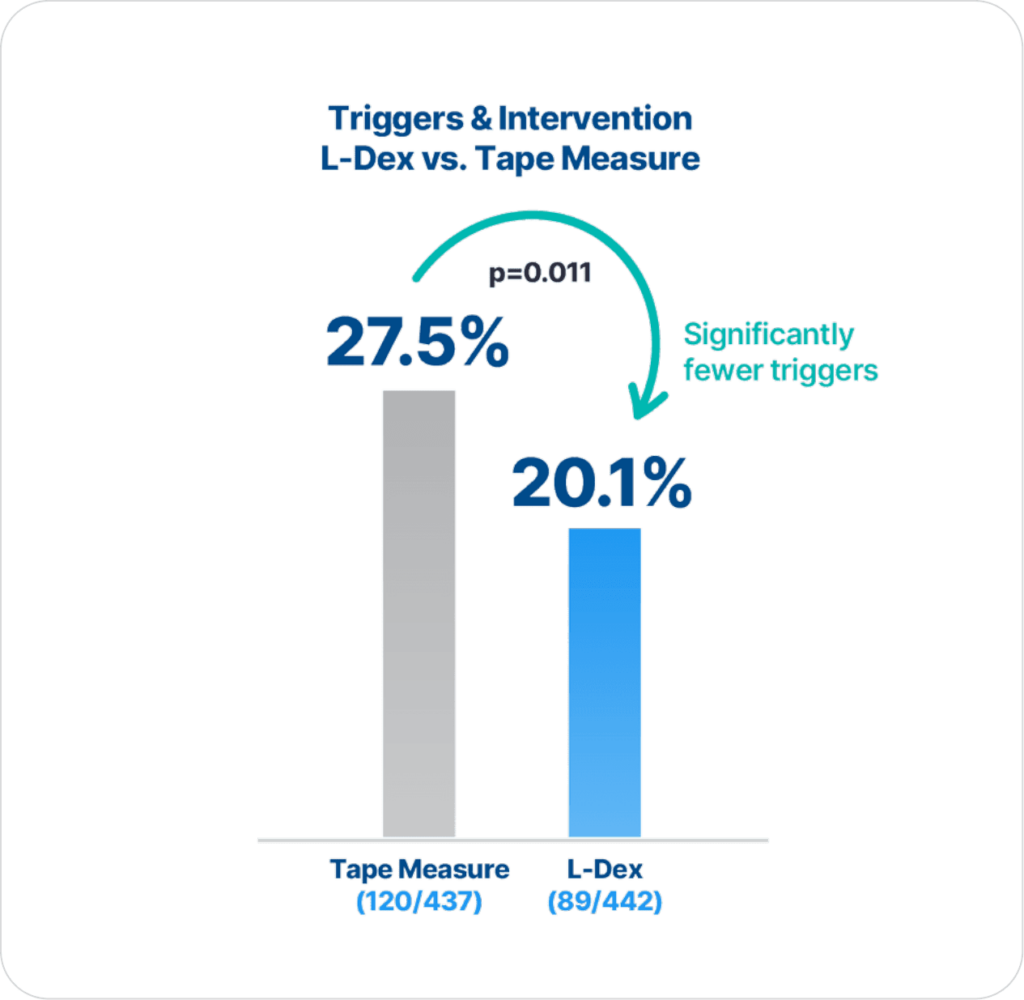
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
Extensive clinical evidence shows that using ImpediMed’s bioimpedance spectroscopy (BIS) technology for early detection and intervention reduces the impact of chronic lymphedema on breast cancer patients.
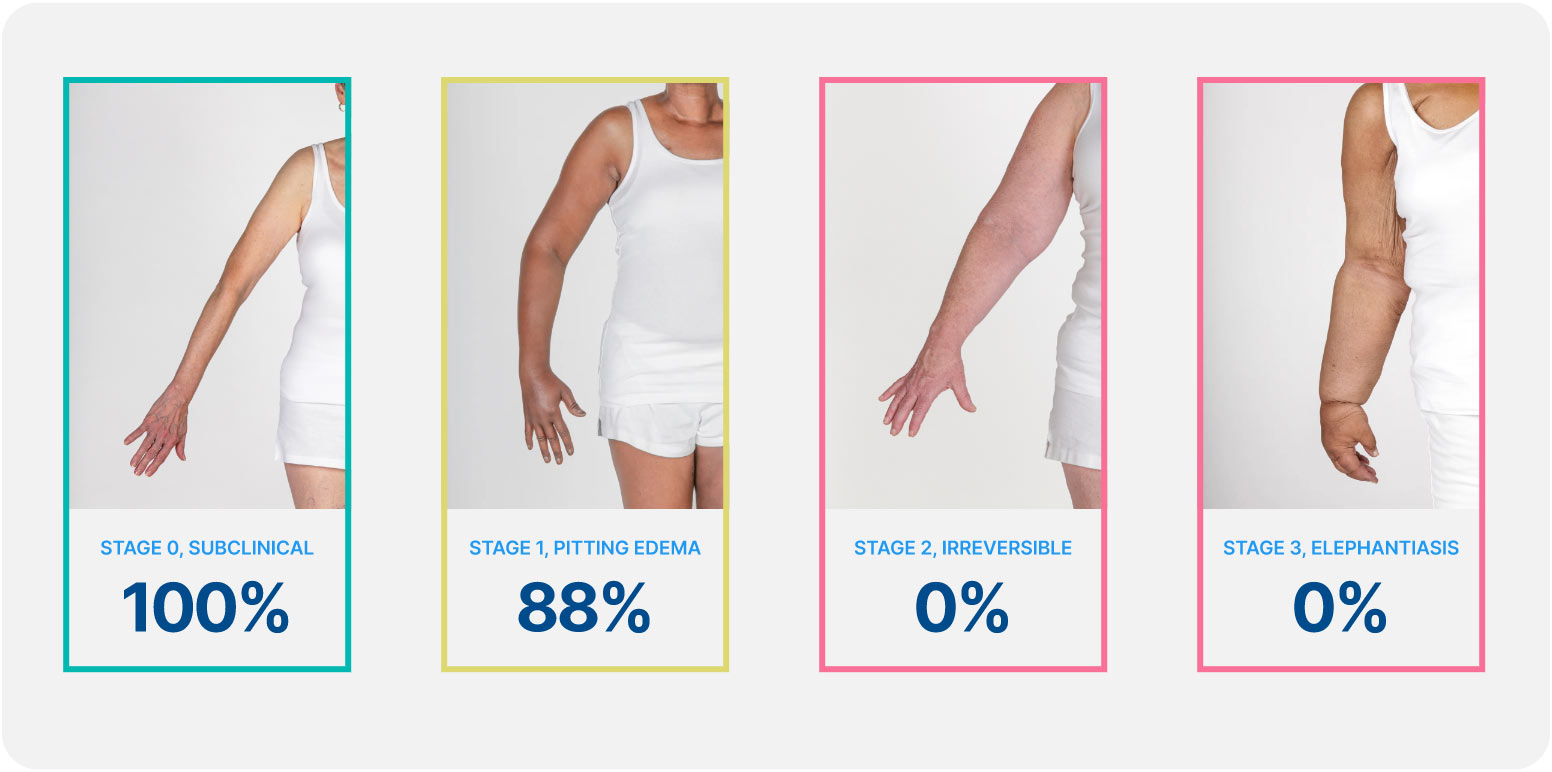
Lymphedema develops in stages, and a university of Kansas study found that when lymphedema is detected at stage 0 or stage 1 it is reversible, but in stages 2 and 3 it is not. These findings demonstrate how early conservative intervention and prospective monitoring with BIS can significantly lower rates of BCRL and persistent BCRL (pBCRL).¹
The PREVENT Trial involved 10 centers across the US and Australia and was the largest randomized controlled trial (RCT) to assess lymphedema prevention in breast cancer patients.
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
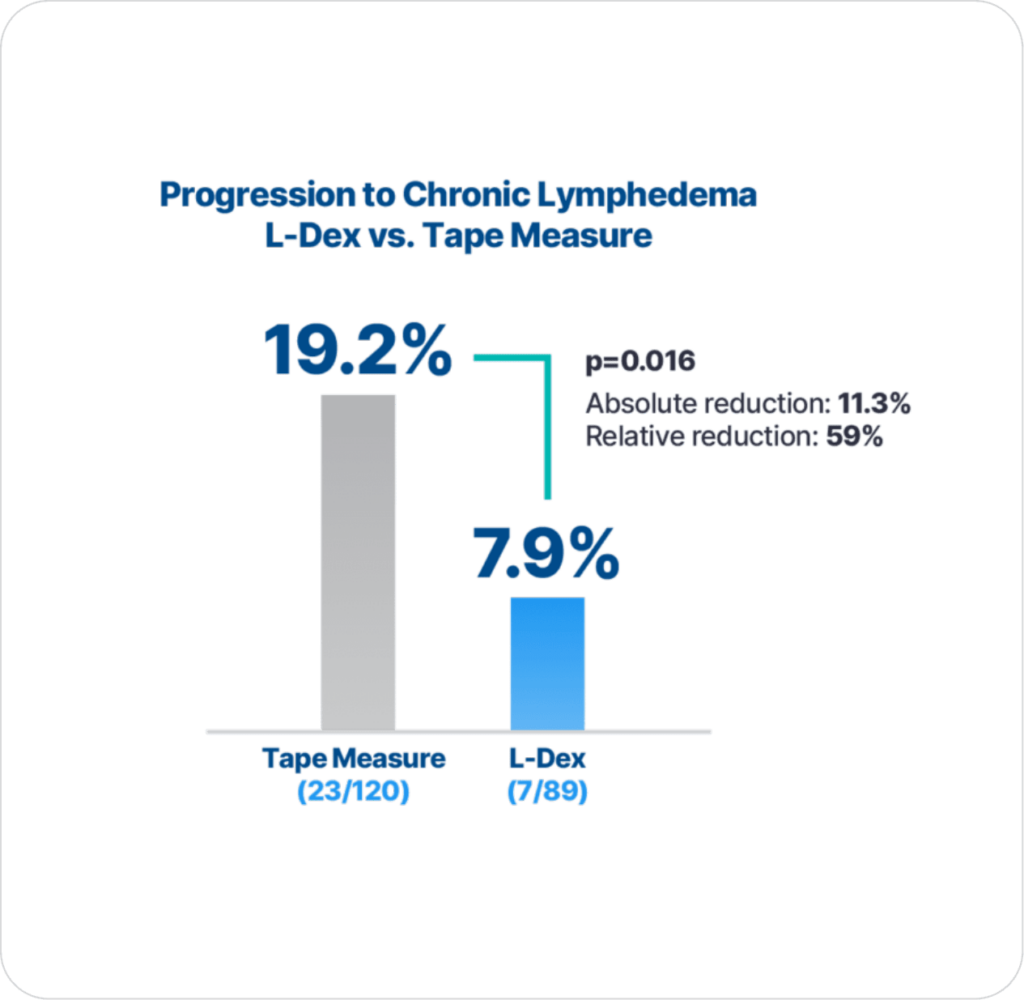
Additionally, with early detection using BIS technology and intervention there is significantly lower progression to chronic lymphedema compared to using tape measure (p=0.016), which is the primary endpoint result2.
Early diagnosis and treatment of lymphedema may mitigate symptoms.
Open access: YesThese data support the need for long-term (24 months) prospective surveillance with frequent assessments (every 3 months) at least 15 months after surgery. Statistically significant convergence of symptom cluster scores with L-Dex unit change supports BIS as beneficial in the early identification of subclinical lymphedema.
From the American Physical Therapy Association, recent guidelines include a prospective surveillance model and early, preventative intervention for patients at risk of cancer-related lymphedema.
Open access: YesBioimpedance spectroscopy as a tool for serial measurement and risk assessment
Open access: YesThe L-Dex ratio correlated with limb volume and clinical assessment of pitting edema, and physiologic measures of lymphatic function, and demonstrated face, construct, and criterion validity in response to intervention. These findings support the adjunctive use of the L-Dex ratio with limb volume measurements for objective diagnosis, evaluation of lymphedema severity, longitudinal serial evaluation of lymphedema, and response to conservative and surgical interventions.
Coroneos, C.J., et al., Correlation of L-Dex Bioimpedance Spectroscopy with Limb Volume and Lymphatic Function in Lymphedema. Lymphat Res Biol, 2018
The results of this interim analysis demonstrate that patients undergoing surveillance with BIS had reduced but non-statistically significant reductions in the rates of progression requiring CDP compared with TM. These results are currently supportive of the need for subclinical detection and early intervention for patients with BCRL, with a 10% absolute reduction and 67% relative reduction in the rates of CDP. Further data with a longer follow-up than in this study is expected in the years to come and will strengthen these early, positive, practice-changing results.
Ridner, S.H., et al., A Randomized Trial Evaluating Bioimpedance Spectroscopy Versus Tape Measurement for the Prevention of Lymphedema Following Treatment for Breast Cancer: Interim Analysis. Ann Surg Oncol, 2019.
Bioimpedance listed under Validated Clinical tools for Diagnosing Lymphedema
Open access: YesScholars and guidelines have advocated for the routine implementation of early lymphedema surveillance and intervention after breast cancer treatment. Regular clinic visits to monitor extracellular fluid present an opportunity for therapists to provide risk management education, psychological support, physical rehabilitation, empowerment, and survivorship care. The findings from the current study support the use of BIS as part of an early prospective surveillance model of care that results in significantly earlier detection of lymphedema over time. Furthermore, the earlier detection of lymphedema will lead to lower health care costs if it results in the effective management of symptoms and prevents progression to severe clinical lymphedema.
Koelmeyer, L.A., et al., Early surveillance is associated with less incidence and severity of breast cancer-related lymphedema compared with a traditional referral model of care. Cancer 2018.
This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the author’s clinical recommendations.
I would recommend a surveillance program that includes quarterly assessment of bioimpedance during this first year after treatment, which is when the majority of cases appear. There should also be prompt use of compression garments and, as necessary, use of decongestive physiotherapy for symptoms or for worrisome changes in bioimpedance.
Open access: NoBioelectrical spectroscopy (BIS) or infrared perometry are suggested as alternative or adjunct methods to circumferential measurement. Specific protocols describing standard positions and measurements for these procedures should be in place.
BIS reading outside normal limits for equipment being used (e.g., L-Dex reading >10) warrant immediate referral for further evaluation by a professional trained in lymphedema assessment and management.
Open access: YesBIS has been shown to provide reliable data to be used in the diagnosis of breast cancer-related lymphedema. BIS can detect early changes associated with lymphedema.
Open access: YesAt the time of breast cancer diagnosis, L-Dex values are similar to normative values. Identified maximum changes in L-Dex values 12 months postoperatively suggest that frequent L-Dex measurements during that time frame are of potential clinical benefit. Our findings are consistent with research supporting an L-Dex value of >7 as indicative of clinical lymphedema with subclinical lymphedema logically occurring at somewhat lower likely, near >6.5.
Ridner, S.H., et al., A Prospective Study of L-Dex Values in Breast Cancer Patients Pretreatment and Through 12 Months Postoperatively. Lymphat Res Biol, 2018. 16(5): p. 435-441