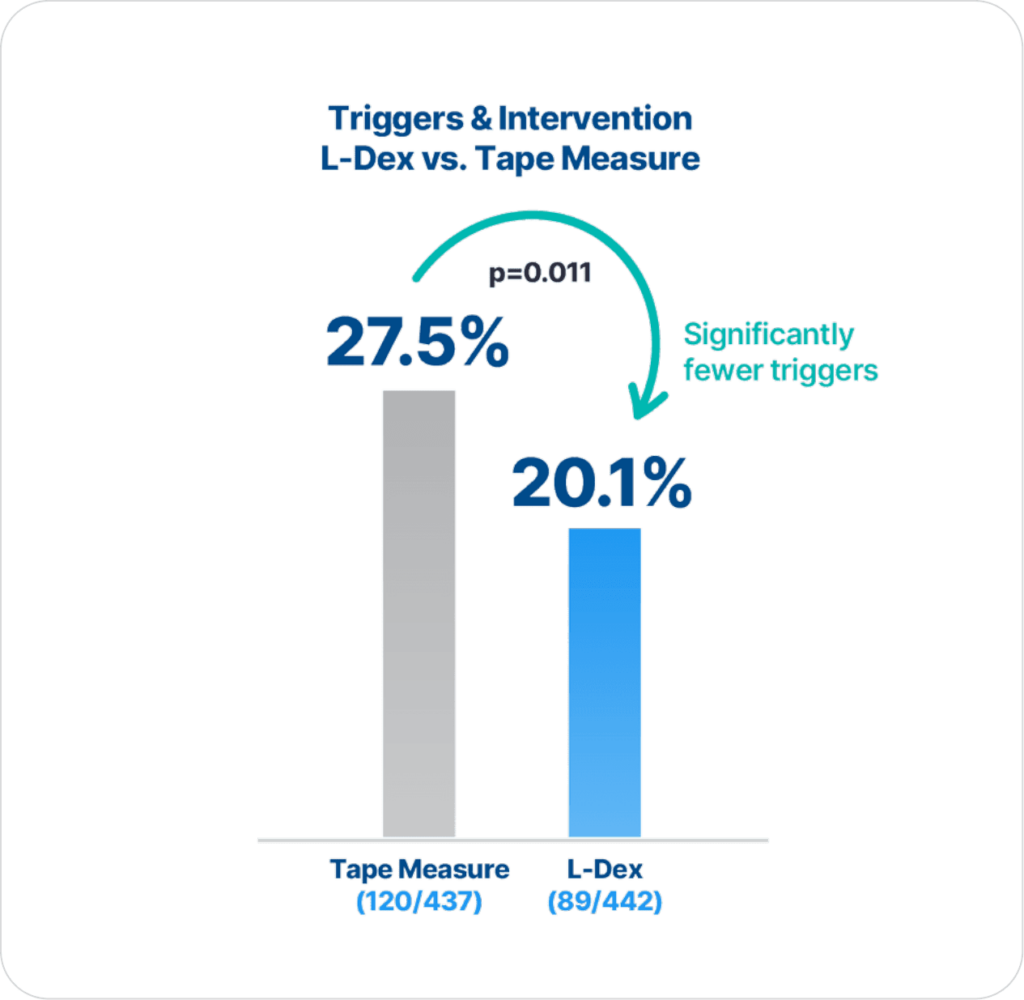
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
Extensive clinical evidence shows that using ImpediMed’s bioimpedance spectroscopy (BIS) technology for early detection and intervention reduces the impact of chronic lymphedema on breast cancer patients.
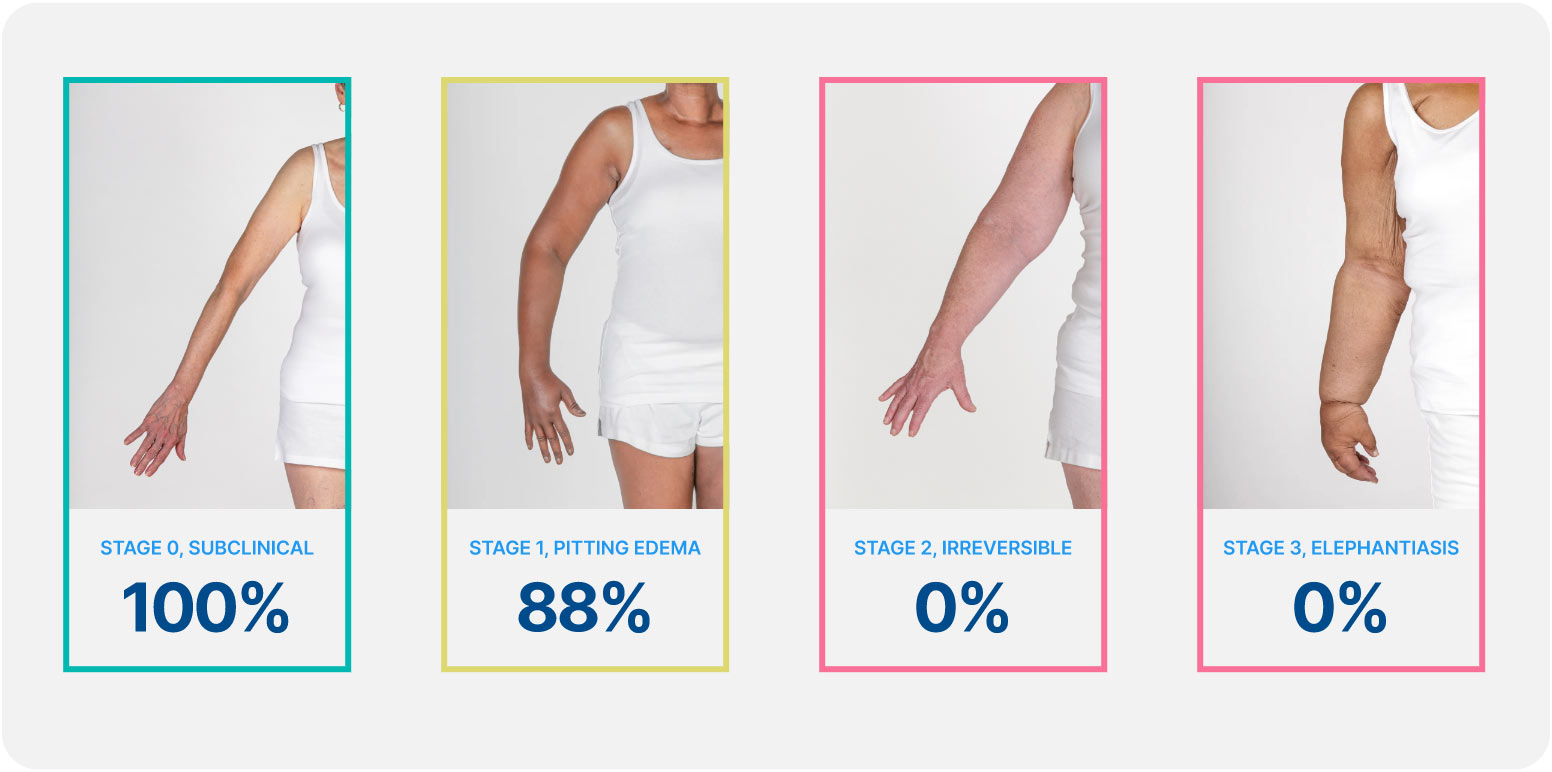
Lymphedema develops in stages, and a university of Kansas study found that when lymphedema is detected at stage 0 or stage 1 it is reversible, but in stages 2 and 3 it is not. These findings demonstrate how early conservative intervention and prospective monitoring with BIS can significantly lower rates of BCRL and persistent BCRL (pBCRL).¹
The PREVENT Trial involved 10 centers across the US and Australia and was the largest randomized controlled trial (RCT) to assess lymphedema prevention in breast cancer patients.
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
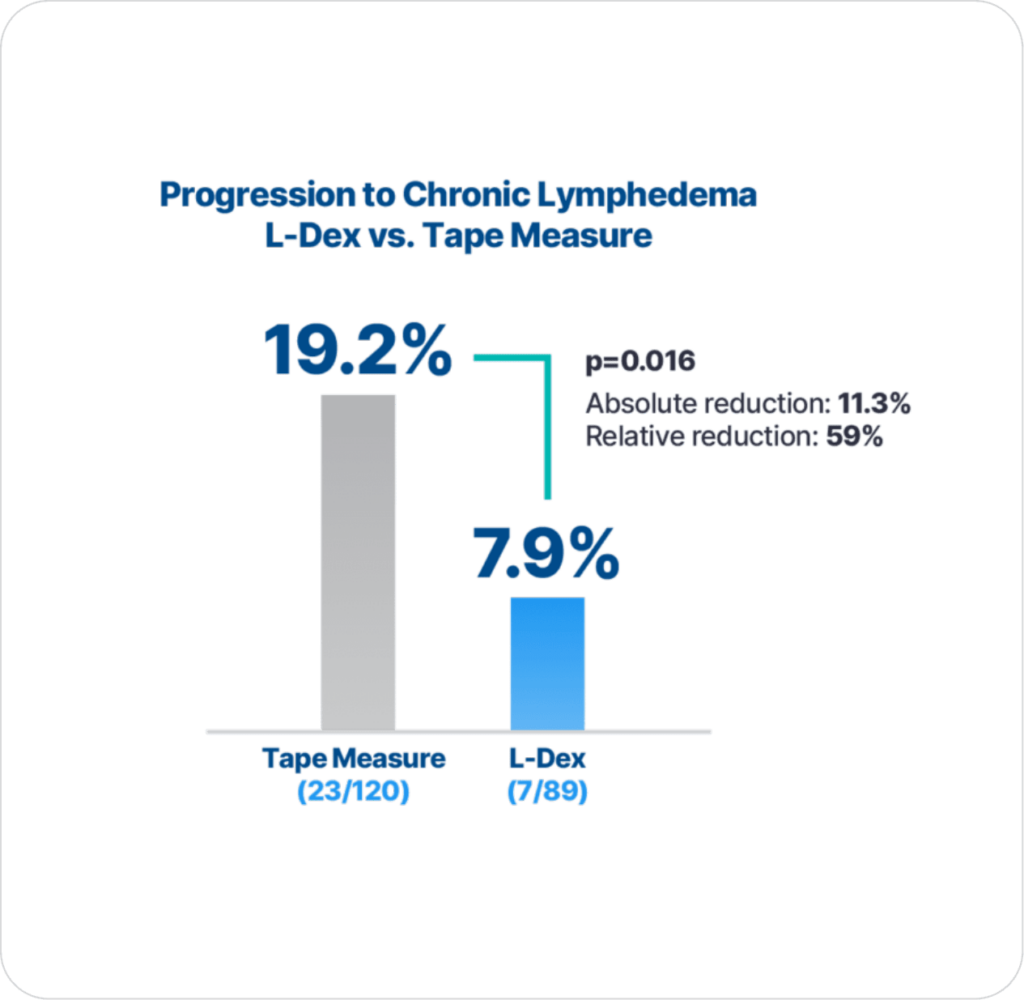
Additionally, with early detection using BIS technology and intervention there is significantly lower progression to chronic lymphedema compared to using tape measure (p=0.016), which is the primary endpoint result2.
These clinical practice guidelines present clinicians with a standardized evidence-based approach to BCRL surveillance to detect subclinical BCRL, allowing for early intervention and low rates of chronic BCRL.
Open access: YesAmerican Society of Breast Surgeons (ASBrS) Lymphatic Surgery Working Group Agrees: Evidence Supports Programs for Early Detection and Intervention to Prevent Chronic Lymphedema.
Open access: YesThe Kaplan–Meier analysis shows that patients with early detection using L-Dex and intervention have statistically significant higher rates of lymphedema progression free survival through three years compared to using tape measure. This reinforces the importance of monitoring patients for three years, since progression to chronic lymphedema occurred throughout the three-year follow up period.
Open access: YesPatients underwent a compression (sleeve and gauntlet) intervention for subclinical breast cancer-related lymphedema (S-BCRL). Physical, emotional, and quality-of-life (QoL) outcomes were examined. Associations of change in extracellular fluid alone through bioimpedance spectroscopy (BIS) or change in whole-arm volume through tape measure with the outcomes at time of S-BCRL were explored.
Open access: YesThe results confirm known BCRL risk factors such as axillary lymph node dissection, taxane-based chemotherapy, regional nodal irradiation, and obesity and provides novel data on the increased risk of BCRL in patients living in a rural areas as well as no increased risk from air travel.
Open access: YesThis study compared rates of progression to chronic breast cancer-related lymphedema (defined as ≥ 10% arm volume change from baseline requiring complex decongestive physiotherapy [CDP]) following an intervention for subclinical lymphedema (S-BCRL) triggered by bioimpedance spectroscopy (BIS) or by tape measurement (TM).
Open access: YesThese data support the need for long-term (24 months) prospective surveillance with frequent assessments (every 3 months) at least 15 months after surgery. Statistically significant convergence of symptom cluster scores with L-Dex unit change supports BIS as beneficial in the early identification of subclinical lymphedema.
The results of this interim analysis demonstrate that patients undergoing surveillance with BIS had reduced but non-statistically significant reductions in the rates of progression requiring CDP compared with TM. These results are currently supportive of the need for subclinical detection and early intervention for patients with BCRL, with a 10% absolute reduction and 67% relative reduction in the rates of CDP. Further data with a longer follow-up than in this study is expected in the years to come and will strengthen these early, positive, practice-changing results.
Ridner, S.H., et al., A Randomized Trial Evaluating Bioimpedance Spectroscopy Versus Tape Measurement for the Prevention of Lymphedema Following Treatment for Breast Cancer: Interim Analysis. Ann Surg Oncol, 2019.
Scholars and guidelines have advocated for the routine implementation of early lymphedema surveillance and intervention after breast cancer treatment. Regular clinic visits to monitor extracellular fluid present an opportunity for therapists to provide risk management education, psychological support, physical rehabilitation, empowerment, and survivorship care. The findings from the current study support the use of BIS as part of an early prospective surveillance model of care that results in significantly earlier detection of lymphedema over time. Furthermore, the earlier detection of lymphedema will lead to lower health care costs if it results in the effective management of symptoms and prevents progression to severe clinical lymphedema.
Koelmeyer, L.A., et al., Early surveillance is associated with less incidence and severity of breast cancer-related lymphedema compared with a traditional referral model of care. Cancer 2018.
Our results demonstrated that early conservative intervention for breast cancer patients high risk for BCRL who were prospectively monitored by utilizing BIS significantly lowers rates of BCRL. These findings support early prospective screening and intervention for BCRL. Early detection with patient-directed interventions improves patient outcomes and decreases the risk of persistent BCRL.
Kilgore, L.J., et al., Reducing Breast Cancer-Related Lymphedema (BCRL) Through Prospective Surveillance Monitoring Using Bioimpedance Spectroscopy (BIS) and Patient Directed Self-Interventions. Ann Surg Oncol, 2018.
The results of this analysis underscore previously published data on the efficacy of prospective BCRL surveillance and early intervention using BIS. Of the 93 high-risk patients prospectively followed and managed in this structured BCRL protocol, only 11% required CDP and only 3% required continued therapy. These excellent outcomes are superior to contemporary studies of conventional measures reporting BCRL rates in similarly treated high-risk patients.
Whitworth, P.W., et al., Preventing Breast Cancer-Related Lymphedema in High-Risk Patients: The Impact of a Structured Surveillance Protocol Using Bioimpedance Spectroscopy. Front Oncol, 2018. 8: p. 197.
In summary, BIS represents a valuable and practical tool for the early detection of subclinical BCRL in patients undergoing prospective monitoring. In this prospective surveillance study, use of BIS allowed for early intervention and a reduction in the predicted rate of chronic BCRL compared to historical controls (no cases of persistent, chronic BCRL were observed after early intervention even in the highest risk patients). Such an approach represents not only a valuable strategy to address the recent NCCN guidelines on survivorship for monitoring for BCRL but also a cost-effective strategy to prevent and manage the potentially devastating effects of chronic BCRL.
Kaufman, D.I., et al., Utilization of bioimpedance spectroscopy in the prevention of chronic breast cancer-related lymphedema. Breast Cancer Res Treat, 2017. 166(3): p. 809-815.