Personalized Exercise
Informs personalized exercise and medical weight management plans.
The SOZO® Digital Health Platform provides precision body composition assessment to monitor key health indicators for patients on medical weight management and lifestyle medicine programs, including GLP-1 therapy and structured exercise and nutrition planning — tracking muscle strength, function, and body composition.1


SOZO with Bioimpedance Spectroscopy (BIS) offers non-invasive precision in tracking fat mass, lean mass and fluid status, all in under 30 seconds:
Informs personalized exercise and medical weight management plans.
Identifies metabolic risks early, including weight gain from endocrine therapy or loss of lean mass from inactivity.
Validates fluid, fat mass, and muscle response to nutritional plans.
This 59-year-old female with Class I Obesity and CAD was monitored with SOZO BodyComp prior to and during initiation of GLP-1/GIP therapy for weight loss.

BMI only reflects total body weight relative to height — it cannot distinguish between fat mass and muscle mass. This distinction is critical for patients on GLP-1 therapies, because weight loss from these medications does not always come from fat alone. Patients can lose significant lean muscle mass and fluid alongside fat, which may go completely undetected when monitoring only with a scale or BMI. The Lancet Diabetes & Endocrinology Commission has noted that traditional measures like BMI should be used only as population-level surrogates for health risk, and that clinical assessment of obesity requires objective measurements — such as direct body fat measurement by bioimpedance. Without body composition monitoring, clinicians may mistake muscle loss for successful fat loss, missing an opportunity to intervene with nutritional or exercise adjustments before the loss becomes clinically significant.
Leading clinical guidelines now recommend baseline and ongoing assessment of lean body mass during weight loss pharmacotherapy, including GLP-1 therapy, using validated tools such as bioimpedance analysis. A joint advisory from The Obesity Society, the Obesity Medicine Association, the American Society for Nutrition, and the American College of Lifestyle Medicine specifically calls for serial lean mass monitoring during GLP-1 treatment. The SOZO® Digital Health Platform with BodyComp™ Analysis uses bioimpedance spectroscopy (BIS) to measure fat mass, skeletal muscle mass, and fluid status in a single non-invasive scan that takes under 30 seconds. This allows clinicians to track whether a patient is preserving muscle during weight loss, identify concerning shifts in body composition early, and tailor exercise and nutrition interventions before muscle loss advances.
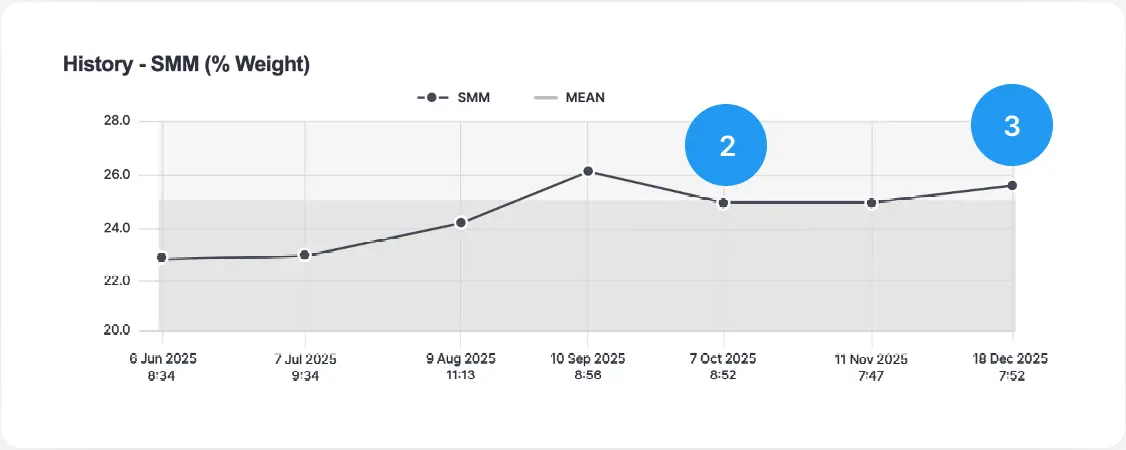
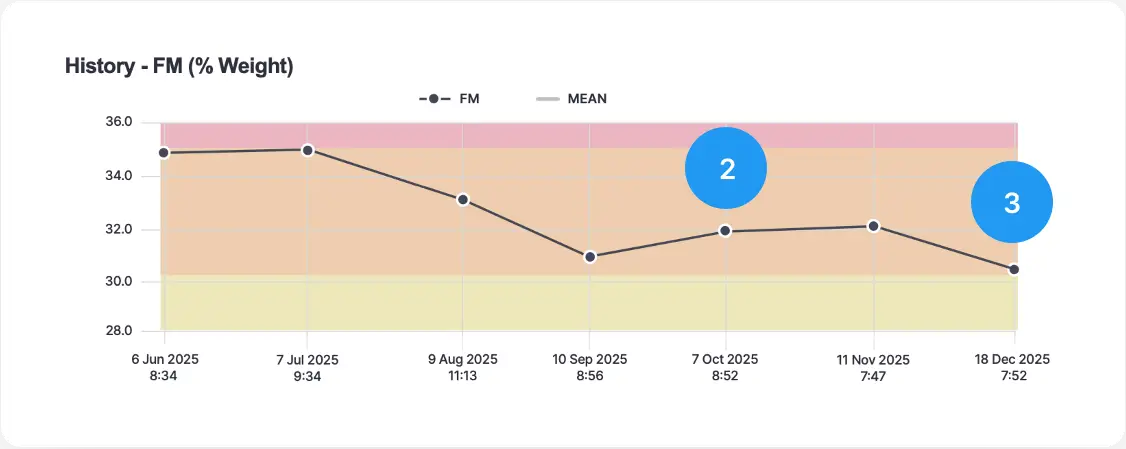
A clinical case documented with the SOZO® platform illustrates exactly what the scale alone can miss. A 59-year-old woman with Class I obesity being treated with GLP-1/GIP therapy lost weight steadily — roughly 0.8 lbs per week — over six months, with her BMI declining consistently throughout. However, BodyComp™ analysis revealed a more nuanced picture: while her skeletal muscle mass percentage was initially increasing and fat mass decreasing, around months four and five this trend reversed, with muscle mass dropping and fat mass rising — even as overall weight continued to fall. This shift was invisible on the scale. Her care team was able to intervene, and by month six her skeletal muscle mass had stabilized and resumed increasing. By the end of the six-month period, her weight had decreased from 188 lbs to 166 lbs while her muscle mass was preserved — an outcome made possible only through objective body composition tracking.
Multiple major clinical bodies now specifically call for objective body composition assessment in structured weight management programs. The Lancet Diabetes & Endocrinology Commission recommends direct measurement of body fat as part of the clinical diagnosis of obesity. A joint advisory from four major nutrition and obesity organizations recommends both baseline and serial measurement of lean body mass during weight loss pharmacotherapy, citing validated bioimpedance tools as appropriate instruments. Additionally, the American College of Surgeons’ MBSAQIP® accreditation standards require accredited obesity medicine programs to capture body fat percentage at initial presentation and track changes over time as part of outcomes monitoring. Taken together, these guidelines establish body composition monitoring — beyond the scale and BMI — as an emerging standard of care in medical weight management.