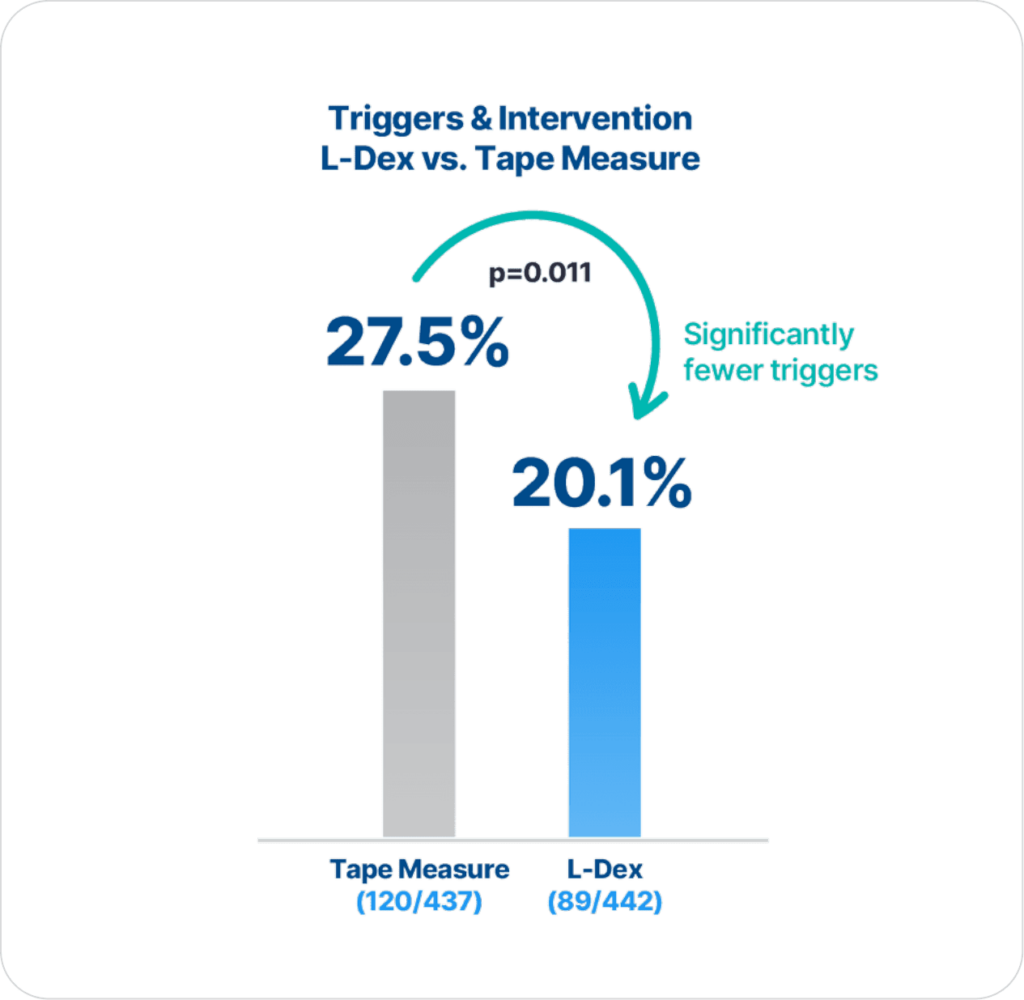
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
Extensive clinical evidence shows that using ImpediMed’s bioimpedance spectroscopy (BIS) technology for early detection and intervention reduces the impact of chronic lymphedema on breast cancer patients.
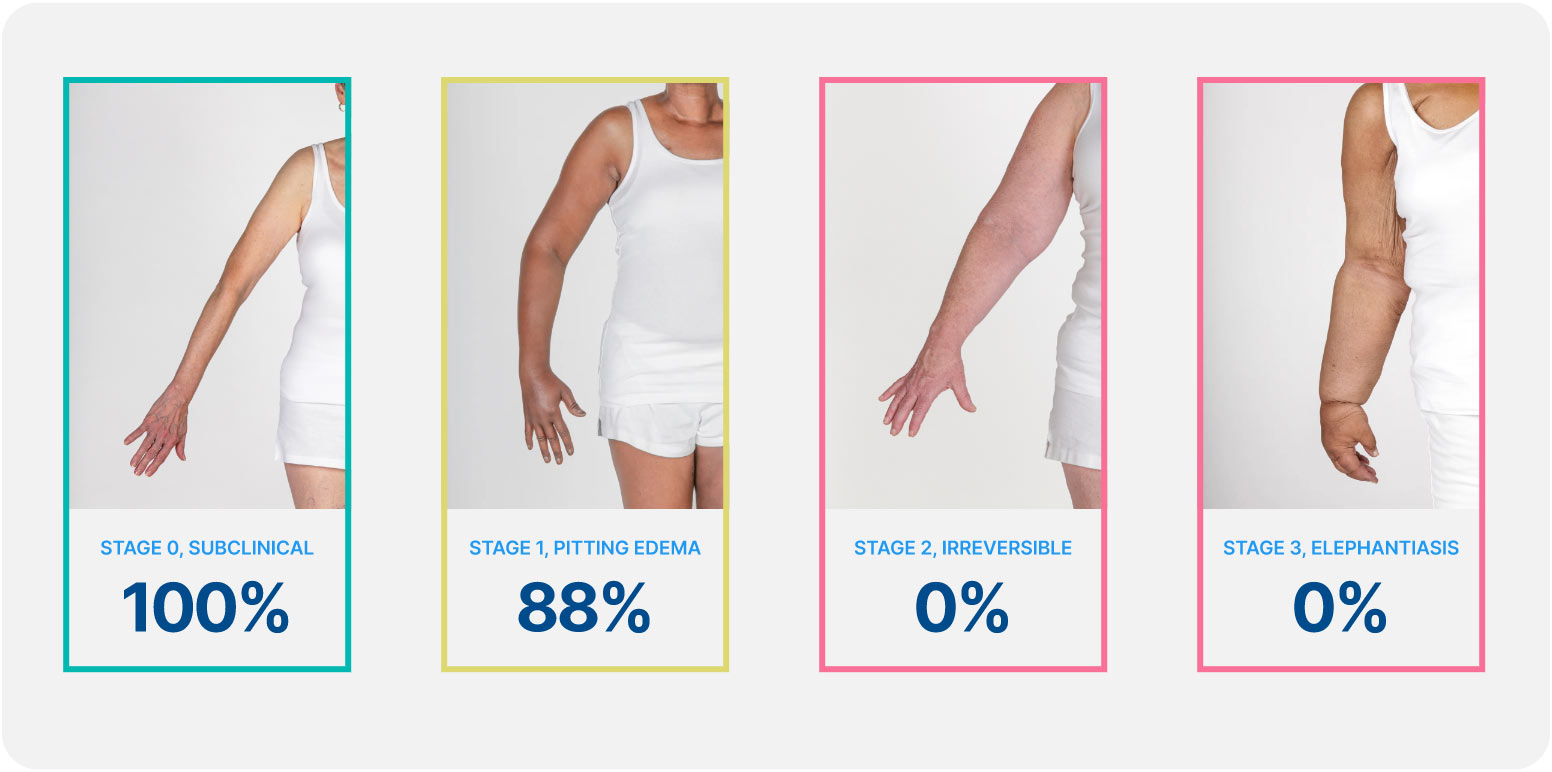
Lymphedema develops in stages, and a university of Kansas study found that when lymphedema is detected at stage 0 or stage 1 it is reversible, but in stages 2 and 3 it is not. These findings demonstrate how early conservative intervention and prospective monitoring with BIS can significantly lower rates of BCRL and persistent BCRL (pBCRL).¹
The PREVENT Trial involved 10 centers across the US and Australia and was the largest randomized controlled trial (RCT) to assess lymphedema prevention in breast cancer patients.
ImpediMed’s BIS technology is more precise and reliable than tape measure in detecting lymphedema (LE), as there are statistically significantly fewer triggers and interventions for those assessed with BIS compared to tape measure (p=0.011)2.
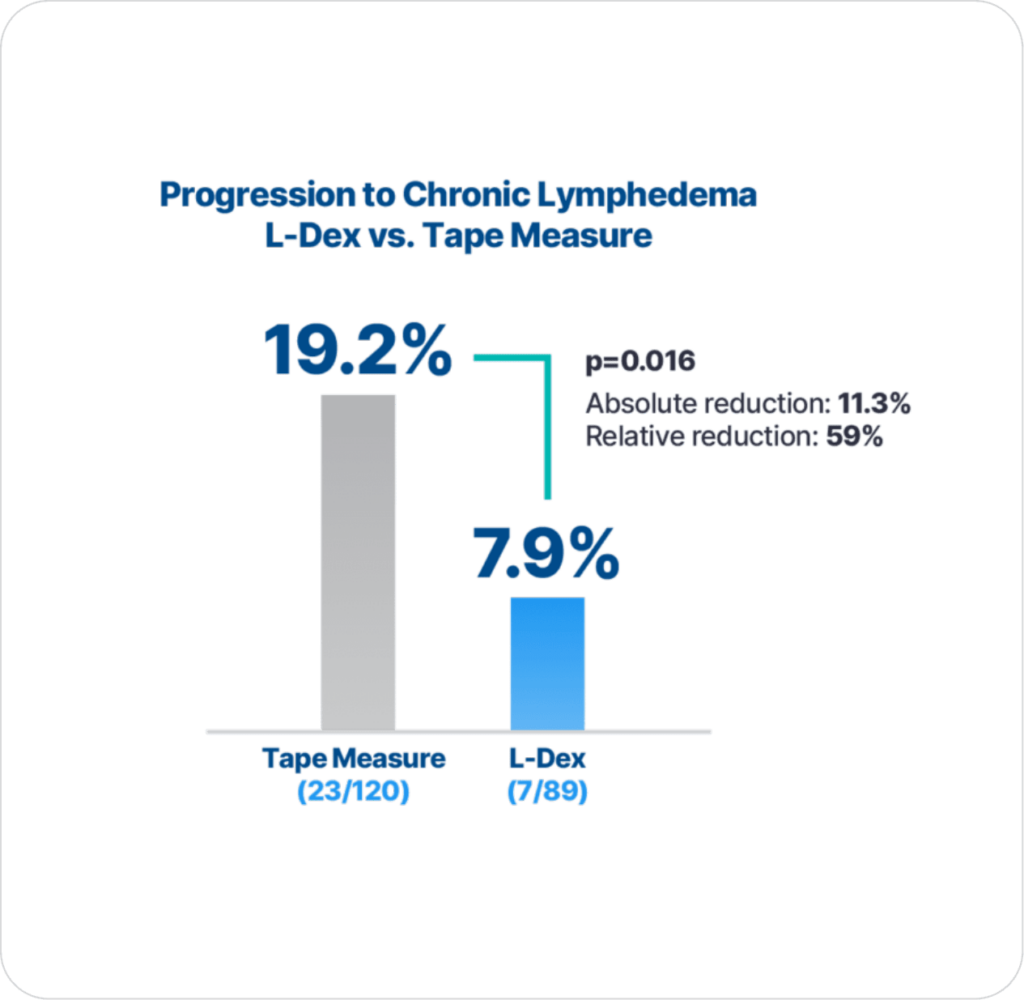
Additionally, with early detection using BIS technology and intervention there is significantly lower progression to chronic lymphedema compared to using tape measure (p=0.016), which is the primary endpoint result2.
Complicated lymphedema was defined as any hospital admission within 2 years for a diagnosis of lymphedema or related complications based on prior research.
This study demonstrates a 2.3% incidence of complicated lymphedema after breast cancer surgery. Increased health care utilization for these patients resulted in hospital charge accrual of more than $180 million in 2 years or approximately $140,000 per patient. Although limitations must be taken into consideration, the significant burden of lymphedema underscored here mandates further investigation into targeted, anticipatory management strategies for BCRL
Basta, M.N., et al., Complicated breast cancer-related lymphedema: evaluating health care resource utilization and associated costs of management. Am J Surg, 2016. 211(1): p. 133-41.
Economic analysis demonstrating that BIS utilization would lead to a cost savings which is magnified when considering sequelae of BCRL.
Over 1 year, BIS-aided assessment of lymphedema for patients following treatment for BC results in cost savings, even without considering potential cost savings associated with averted downstream sequelae.
Bilir, S.P., M.P. DeKoven, and J. Munakata, Economic benefits of BIS-aided assessment of post-BC lymphedema in the United States. Am J Manag Care, 2012. 18(5): p. 234-41.
Early intervention may reduce the need for intensive rehabilitation and may be cost saving. This perspective article compares a prospective surveillance model with a traditional model of impairment-based care and examines direct treatment costs associated with
each program.
The prospective surveillance model includes the cost of screening all women plus the cost of intervention for early-stage BCRL. The TM group comprised women referred for BCRL treatment using a traditional model of referral based on late-stage lymphedema. The
traditional model cost includes the direct cost of treating patients with advancedstage lymphedema. The cost to manage early-stage BCRL per patient per year using a prospective surveillance model is $636.19. The cost to manage late-stage BCRL per patient per year using a traditional model is $3,124.92. The prospective surveillance model is emerging as the standard of care in breast cancer treatment and is a potential cost-saving mechanism for BCRL treatment.
Stout, N.L., et al., Breast cancer-related lymphedema: comparing direct costs of a prospective surveillance model and a traditional model of care. Phys Ther, 2012. 92(1): p. 152-63
Claims study of 1,877 patients for 2 years after the start of cancer treatment. 10% of patients developed lymphedema with ALND and chemotherapy associated with development. Higher medical costs associated with BCRL diagnosis ($23, 167 vs. $14,877) with higher rates of cellulitis/lymphangitis noted.
Although the use of claims data may underestimate the true incidence of lymphedema, women with BCRL had a greater risk of infections and incurred higher medical costs. The substantial costs documented here suggest that further efforts should be made to elucidate reduction and prevention strategies for BCRL.
Shih, Y.C., et al., Incidence, Treatment Costs, and Complications of Lymphedema After Breast Cancer Among Women of Working Age: A 2-Year Follow-Up Study. J Clin Oncol, 2009.